

Radial Tunnel Syndrome
What is radial tunnel syndrome?
Radial tunnel syndrome happens when the radial nerve is squeezed where it passes through a tunnel near the elbow.
What is the radial tunnel?
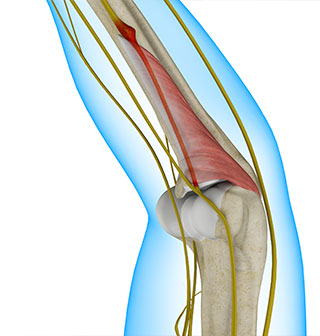
The radial nerve starts at the side of the neck, where the individual nerve roots leave the spine. The nerve passes down the back of the upper arm. It then spirals outward and crosses the outside (the lateral part) of the elbow before it winds its way down the forearm and hand. On the lateral part of the elbow, the radial nerve enters a tunnel formed by muscles and bone. This is called the radial tunnel.
Passing through the radial tunnel, the radial nerve runs below the supinator muscle. The supinator muscle lets you twist your right hand clockwise. This is the motion of using a screwdriver to tighten a screw. After the radial nerve passes under the supinator muscle, it branches out and attaches to the muscles on the back of the forearm.
What causes radial tunnel syndrome?
Pain is caused by pressure on the radial nerve. There are several spots along the radial tunnel that can pinch the nerve. If the tunnel is too small, it can squeeze the nerve and cause pain. Repetitive, forceful pushing and pulling, bending of the wrist, gripping, and pinching can also stretch and irritate the nerve. Sometimes a direct blow to the outside of the elbow can injure the radial nerve. Constant twisting movements of the arm, common in assembly work, can also pinch the radial nerve and lead to radial tunnel syndrome.
What are the symptoms?
The symptoms of radial tunnel syndrome are tenderness and pain on the outside of the elbow. The symptoms of radial tunnel syndrome are very similar to the symptoms of tennis elbow. As in tennis elbow, pain from radial tunnel syndrome often starts near the lateral epicondyle. (The lateral epicondyle is a bony point on the outside of your elbow joint.) The pain gets worse when you bend your wrist backward, turn your palm upward, or hold something with a stiff wrist or straightened elbow. One difference between radial tunnel syndrome and tennis elbow is the exact location of the pain. In tennis elbow, the pain starts where the tendon attaches to the lateral epicondyle. In radial tunnel syndrome, the pain is centered about two inches further down the arm, over the spot where the radial nerve goes under the supinator muscle. Radial tunnel syndrome may also cause a more achy type of pain or fatigue in the muscles of the forearm. Nerve pressure inside the radial tunnel leads to weakness in the muscles on the back of the forearm and wrist, making it difficult to steady the wrist when grasping and lifting. It can even lead to wrist drop, meaning the back of the hand can't be cocked up. Skin sensation is not changed because the sensory portion of the radial nerve branches off above the elbow and does not enter the radial tunnel.
How is it diagnosed?
The diagnosis of radial tunnel syndrome can be difficult. Many cases are initially diagnosed as tennis elbow. Tests don't always help tell the two conditions apart. Your doctor will take a detailed medical history. You will be asked questions about your pain, your activities, and any past injuries to your elbow. Your doctor will then do a physical examination to look for the most tion painful spot. Pinpointing the source of the pain will be most helpful in determining whether you have radial tunnel syndrome or tennis elbow.
You may do some tests of the radial nerve. An electromyogram (EMG) tests to see if the muscles of the forearm are working properly. If the test shows a problem with the muscles, it may be caused by a problem with the radial nerve. However, many people who have radial tunnel syndrome will still have normal test results. Your doctor will consider all parts of the examination in diagnosing whether or not you have a problem with radial tunnel syndrome.
What is the treatment?
Treating radial tunnel syndrome can be frustrating, for you and your doctor. Getting your symptoms under control and helping you regain the use of your elbow can be a challenge.
Nonsurgical Treatment:
The most important part of your treatment is to avoid the activity that caused the problem in the first place. You need to avoid repetitive activities that require your wrist to be repeatedly bent backwards. Repeated use of the wrist in twisting motions (such as using a screwdriver) also make the problem worse. If your work tasks caused your condition, you need to modify your work site or your duties. This is crucial for treatment to be successful. You need to take frequent breaks as you work and play. You also need to limit heavy pushing, pulling, and grasping. If symptoms are worse at night, you may want to wear a lightweight plastic arm splint while you sleep. This limits your elbow movements at night and eases further irritation. This may let the elbow rest, giving the nerve time to recover from irritation and pressure. Doctors commonly refer their patients with radial tunnel syndrome for physiotherapy. At first, your therapist will give you tips on how to rest your elbow and how to do your activities without putting extra strain on your elbow. Your therapist may apply ice and electrical stimulation to ease pain. Exercises are used to gradually stretch and strengthen the forearm and muscles.
Surgical treatment:
Sometimes symptoms of radial tunnel syndrome aren't relieved, even after many months of nonsurgical treatment. In these cases, surgery may be the best treatment option. It is generally considered a last resort. The goal of surgery for radial tunnel syndrome is to relieve any abnormal pressure on the nerve where it passes through the radial tunnel. The surgeon begins by making an incision along the outside of the elbow and down the forearm, near the spot where the radial nerve goes under the supinator muscle. Soft tissues are gently moved aside so the surgeon can check the places where the radial nerve may be getting squeezed within the radial tunnel. The nerve can be pinched in many spots, so it is important to check all the areas that may be causing problems. Any parts of the tunnel that are pinching the nerve are cut. This expands the tunnel and relieves pressure on the nerve. At the end of the procedure, the skin is stitched together.